
What is periodontitis?
Gum disease (periodontitis) refers to an infection-induced inflammatory process involving tooth-supporting structures.
Approximately 5% to 20% of any population suffers from severe generalised periodontitis, even though moderate periodontal disease affects a majority of adults. This most common human oral disease is caused by certain bacteria which start to increase in number and virulence when the related risk factors, such as multiplying bacterial deposits, can grow undisturbed under the unreachable gum pockets while producing by-products which may stimulate the body’s defensive inflammatory response in the around the teeth. This chronic inflammatory disease may progress and cause gradual bone destruction over the years when not treated efficiently.
How can the progression of periodontitis be recognised?
The inflamed swollen gum called gingivitis may be recognised during brushing when bleeding. In some individuals, gingivitis may progress to gum disease (periodontitis) when untreated. Consequently, over time, the affected patient may experience increased gum bleeding, bad breath, drifting teeth, gum recession, and tenderness in the gum. Controversially, bleeding from the gums may be less noticeable in smokers, as nicotine has an adverse vasoconstrictive effect on blood vessels by decreasing the local blood circulation, hence reducing bleeding from diseased gum. As periodontitis is usually pain-free, it can be left unrecognised until its very progressed stages. Therefore, to treat periodontitis in a timely manner, it is paramount that dental clinicians, in particular the gum specialist or periodontist, investigate the specific clinical signs and symptoms and radiographic features of gum disease at an early stage of its progressive destruction.
Is periodontitis correlated to other systemic chronic inflammatory diseases?
Based on the case studies, clinical research, and epidemiological studies, there are strong evidenced-based associations between chronic gum infection or periodontal disease and cardiovascular disease (CVD), Alzheimer’s disease, erectile dysfunction syndrome, low-weight child disease, and premature parturition.Read more on the correlation between Periodontal and other systemic inflammatory diseases, e.g., cardiovascular diseases.
Causes of Periodontitis
Retention or accumulation of dental plaque around the teeth may gradually enhance the number and virulence of the bacterial colonies, which may, in turn, reduce the natural defence system of the local tissue. The salivary minerals and gingival crevicular fluid may gradually cause sedimentation of growing bacterial plaque and the creation of harder deposits called tartar or dental calculus. This bacterial growth is further facilitated along the root surfaces, causing an inflammatory process which destroys the peripheral periodontal tissues via the gum pockets. This bacterial infection-induced inflammatory process, which causes progressive destruction of the tooth-supporting/periodontal tissues, is called periodontitis.
The pathologic pocket around the root surface favours the colonisation, growth and multiplication of the virulent bacteria, which are capable of destructing the tissues both directly by releasing destructing enzymes, toxins and other bi-products which compromise the body’s defence mechanisms and indirectly by inflammatory stimulation of the local immune system.
Read more about the diagnosis and treatment of periodontal disease.
Prevention of the Periodontal Disease
The risk factors involved in the emergence and progression of periodontitis could be divided into the local virulent factors, e.g., the number and type of virulent bacteria, the host factors, such as the ability of the individual’s local and systematic defence mechanisms coupled with the tissue healing capacity, the presence of the confounding risk factors which compromise the host response, e.g. smoking, certain drugs regulating the tissue response as well as inherent immune-suppressive factors such as stress, systematic disease. Factors prevailing in chronic gingivitis should be recognised and addressed during professional dental and periodontal examinations and treatment sessions.
It is scientifically well-proved that smoking adversely affects the status of the local health, healing, and immune response of periodontal tissues and the successful treatment of gum disease as a result.
Treatment of Periodontitis
With careful assessment and treatment, it is usually possible to completely halt the progress of periodontitis. The key to success is to eliminate the bacterial plaque triggering the periodontal disease process and establish excellent oral hygiene practices.
At London Specialist Dentist, we provide the following periodontal specialist services:
• Clinical assessment, diagnosis, and treatment of the patient with aggressive and chronic periodontitis.
• Diagnosis and treatment planning for patients with the oral manifestation of systemic disease.
• Clinical assessment, diagnosis, and treatment of patients who require post/endodontic and/or pre-prosthodontic root amputation and crown lengthening.
• Clinical assessment, diagnosis, and treatment of young patients who require pre-orthodontic surgical tooth exposure and patients who require post-orthodontic surgical soft tissue and hard tissue regenerative procedures.
• Clinical assessment, diagnosis, and treatment of patients with clinical periodontal disease symptoms in need of occlusal re-organization by means of fixed and removable prosthodontics.
• Clinical assessment, diagnosis, and treatment of patients presenting with peri-implantitis.
At London Specialist Dentist, we implement triple-wavelength technology in dentistry using the latest generation of LASER. The Laser Infrared wavelength is effectively used in the decontamination of infected periodontal, peri-implant pockets, and infected root canals as an adjunct to the mechanical and chemical debridement within the periodontal, peri-implant and Endodontic treatment protocols. This means the indication for adjunct use of antibiotics and their consequent side effects is drastically reduced.
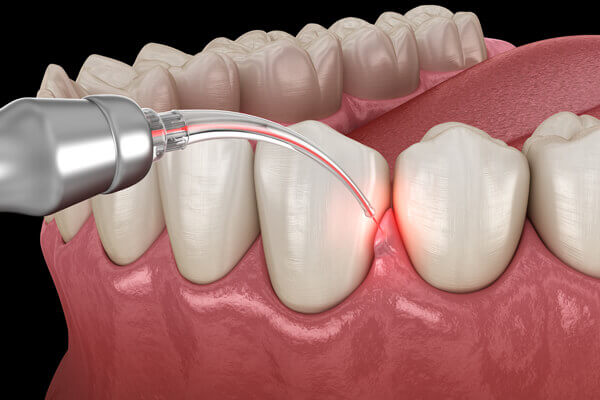
At London Specialist Dentist, we implement the innovative technology of laser-assisted periodontal therapy (LAPT) to improve periodontal health with minimal discomfort following both non-surgical and surgical periodontal treatment interventions. During endodontic treatment, LASER is utilised after preparing and rinsing the root canal in addition to the conventional treatment.
What is gum depigmentation?
Darker gums or gingival hyper-pigmentation can also be hereditary or genetically predisposed in some specific races with darker skins. Another local cause of gum discolouration is the impregnation or absorption of micro-particles from the leaking amalgam (silver) filling into the gum.
What is the treatment for gum depigmentation?
FAQ – What do patients usually ask about periodontology?
CVD encompasses a variety of cardiovascular pathologies, such as angina pectoris, myocardial infarction, and heart failure, as a result of inflammatory processes caused by atherosclerosis.
Atherosclerosis causes a compromised natural blood flow to the heart and increases strain on the heart, manifesting symptoms of CVD, including intense chest pain, breathlessness, dizziness, and fatigue.
Based on the consensus report of periodontitis and cardiovascular disease (CVD), periodontal pathogenic bacteria could induce the development of atherosclerosis in the form of deposit stagnation along cardiac inner blood vessel walls, hence reduced vascular diameter and eventually vascular occlusion.
Atherosclerosis causes a compromised natural blood flow to the brain. A temporary disruption of the brain blood supply may lead to a transient ischaemic attack and, when prolonged, to stroke.
If you have any concerns about the health of your gums or potential periodontal issues, it’s essential to schedule an appointment with a qualified periodontist and gum specialist.
Periodontology Case Studies
See our periodontology before and after photos from our happy patients.

Before and After Treatment
Treated advanced generalised periodontitis followed by restorative correction of the advanced gum recession.
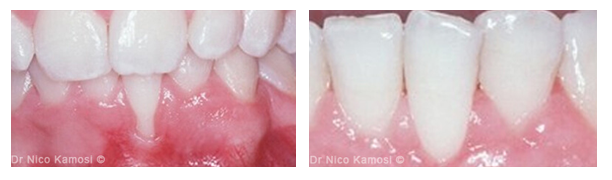
Before and After Treatment
Thin periodontal biotype, gingival recession, reduced vestibular depth, aberrant frenum/muscle pull, exposed root surface.