
Diagnosis of peri-implant disease
Osseointegration is a process by which a clinically asymptomatic rigid direct fixation between an alloplastic material (implant) and surrounding living bone is achieved and maintained under functional loading (Zarb & Albrektsson 1991). One of the key factors in the long-term success of dental implants is maintaining healthy tissues around them.
Peri-implant disease is a collective term for inflammatory reactions in the surrounding tissue of the functioning implant. Peri-implant mucositis is a term describing reversible inflammatory reactions in the surrounding soft tissue of a functioning implant. Simultaneously, peri-implantitis refers to inflammatory reactions with loss of bone supporting functioning implant (Albrektsson & Isidor 1994). The disease of peri-implant mucositis has been shown to occur in about 80% of subjects with an endosseous dental implant (50% of sites).
Peri-implantitis has been defined as a progressive inflammatory bacterial- infectious process deteriorating and destructing the supporting soft and hard tissues around functional osseointegrated implant eliciting bacterial, clinical and radiographic signs and symptoms, e.g. bleeding and suppuration (Mombelli et al. 1987). A cause-effect relationship between bacterial plaque accumulation and the development of inflammatory changes in the soft tissues surrounding dental implants has been shown (Pontoriero 1994). The existing scientific evidence demonstrates a direct association between oral microbiota and bacterial peri-implant inflammatory lesions in the form of Peri-implant mucositis or peri-implantitis.
In both experimental research and human trials (Lang et al. 2000), it has been demonstrated that prolonged accumulation of bacterial plaque over a long period of time may develop the reversible nature of peri-implant mucositis into the irreversible peri-implantitis rendering such complications either amenable to treatment (ailing) or untreatable (failing).
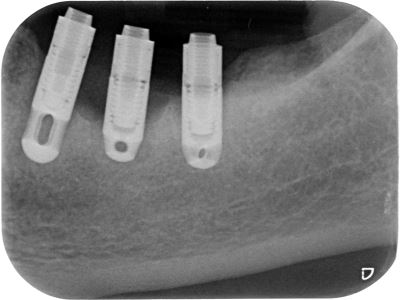
Diagnosis of the peri-implant disease requires a thorough clinical examination to verify the extent and severity of relevant pathological parameters, e.g., bleeding on probing and suppuration combined with deepened Peri-Implant Pocket Depth (PIPD) and radiographic signs of Marginal Bone Loss (MBL). Baseline probing measurements (PIPD) and radiographs should be obtained once the implant’s final restoration is processed and fitted to follow up longitudinal monitoring of peri-implant conditions. Radiographic examinations should be standardized and acquired by reliable techniques and compared with the baseline measurements. The diagnostic procedure and interceptive treatment of destructive peri-implantitis should be attempted at the earliest stage of disease progression.
Clinical and radiographic examination required to determine the presence of peri-implantitis
The assessment of the presence of classical signs and symptoms of inflammation
The radiographic evaluation and evidence of alveolar bone loss following initial healing and bone remodelling.
Standardized radiographs should be taken and compared to reference radiographs taken at the time of prosthesis insertion.
The body of evidence from the recent literature suggests that poor oral hygiene, history of periodontitis, uncontrolled diabetes and heavy smoking, compromised host tissues or immune response, poor bone quality, bone grafting, irradiation therapy, parafunctional activities, the degree of surgical trauma, bacterial contamination, compromised host tissues or immune response along with excessive loading, unfavourable number, distribution, surface characteristics and design of the supporting implants to be associated with biological failures of oral implants. Therefore, the above-mentioned risk factors, especially the standard of oral hygiene, should be reinforced. The periodontal tissues’ general health status around the remaining teeth should be monitored during the maintenance phase.
Peri-implant treatment strategies
A plethora of literature published so far represents insufficient evidence for the effectiveness of advocated treatment modalities of peri-implantitis. The synopsis of accumulated data from experimental research and clinical experience may classify such treatment strategies into 2 main categories:
Non-surgical therapeutic strategies:
The implementation of non-surgical mechanical and adjunctive use of local/systemic antimicrobials therapy to reduce the inflammation has been proved to be effective in the resolution of peri-implant mucositis lesions but unpredictable in the effective treatment of advanced peri-implantitis lesions with a prevalence of 12-40% of sites, in 28%-56% of individuals.
The literature review on the various nonsurgical treatment strategies for peri-implant lesions in animal research and human studies provides evidence that most of the nonsurgical treatment modalities directed to reduce the submucosal infection may result in a short-term improvement of peri-implantitis.
Surgical therapeutic strategies:
The aims and objectives of surgical therapeutic strategies involved in the treatment of peri-implantitis:
- Elimination of the peri-implant granulation tissues.
- Eradication of the interfacial biofilm employing mechanical surface debridement (e.g. ultrasonic, carbon or plastic curettes, air abrasive).
- Decontamination of the infected interface via non-mechanical surface decontamination techniques (e.g. laser devices, adjunctive local sustained-delivery antimicrobial agents, systemic antibiotics alone or in combination).
- Modification of the implant surface architecture to eliminate the micro-mechanical retention niche for pathogenic micro-organisms via resection (implantoplasty).
- Bio-surface modification to promote re-osseointegration (e.g. EDTA., BMP, L-PRF).
- Restoration/ regenerative of the peri-implant lesion.
The extent and quality of bone regeneration and Osseo-reintegration at the interface following the regenerative treatment of peri-implantitis lesions have been variable in various trials and case reports. This could be because the currently advocated regenerative techniques are not performed consistently according to the appropriate clinical protocols and specific indication criteria to perform sufficient debridement, elimination of the residual debris, and effective interface decontamination.
The current treatment modalities advocated in treating peri-implantitis have been reported to exert some beneficial and successful effect. However, up to the present, none of the advocated therapeutic strategies in treating advanced peri-implantitis with specific morphology, extent, and severity has proved to be the most efficacious. Incomplete debridement and surface decontamination seem to be the major obstacle to resolving the lesion and bone regeneration at the implant-tissue interface.
Conclusion: These findings consistently indicate that up to the present, there is no specific individual or combination treatment strategy that has yet been recognised as a gold standard approach for the treatment of peri-implantitis and that the currently available evidence does not specify the superiority of each technique in certain sub-type of peri-implantitis.
The synopsis from 2017 WORLD WORKSHOP: Peri-implant health, peri-implant mucositis, and peri-implantitis:
Case definitions and diagnostic considerations
Stefan Renvert | G. Rutger Persson | Flavia Q. Pirih | Paulo M. Camargo
Peri-implant health: Case definition
Absence of visual peri-implant signs of inflammation (redness, puss, swelling)
Lack of profuse bleeding/or suppuration on probing
Stable peri-implant probing depth in the absence of further bone loss following initial healing (≤2 mm).
Peri-implant mucositis: Case definition
Presence of visual peri-implant signs of inflammation (redness, puss, swelling)
Presence of profuse bleeding/or suppuration on probing
Increased peri-implant probing depth in the absence of peri-implant marginal bone loss following initial healing and remodelling (≤2 mm).
Peri-implantitis: Case definition
- Presence of visual peri-implant signs of inflammation (redness, puss, swelling)
- Presence of profuse bleeding/or suppuration on probing
- Increased peri-implant probing depth
- Presence of peri-implant marginal bone loss following initial healing and remodelling